

BEAS State Registry Consent Form
When completing the form, please include
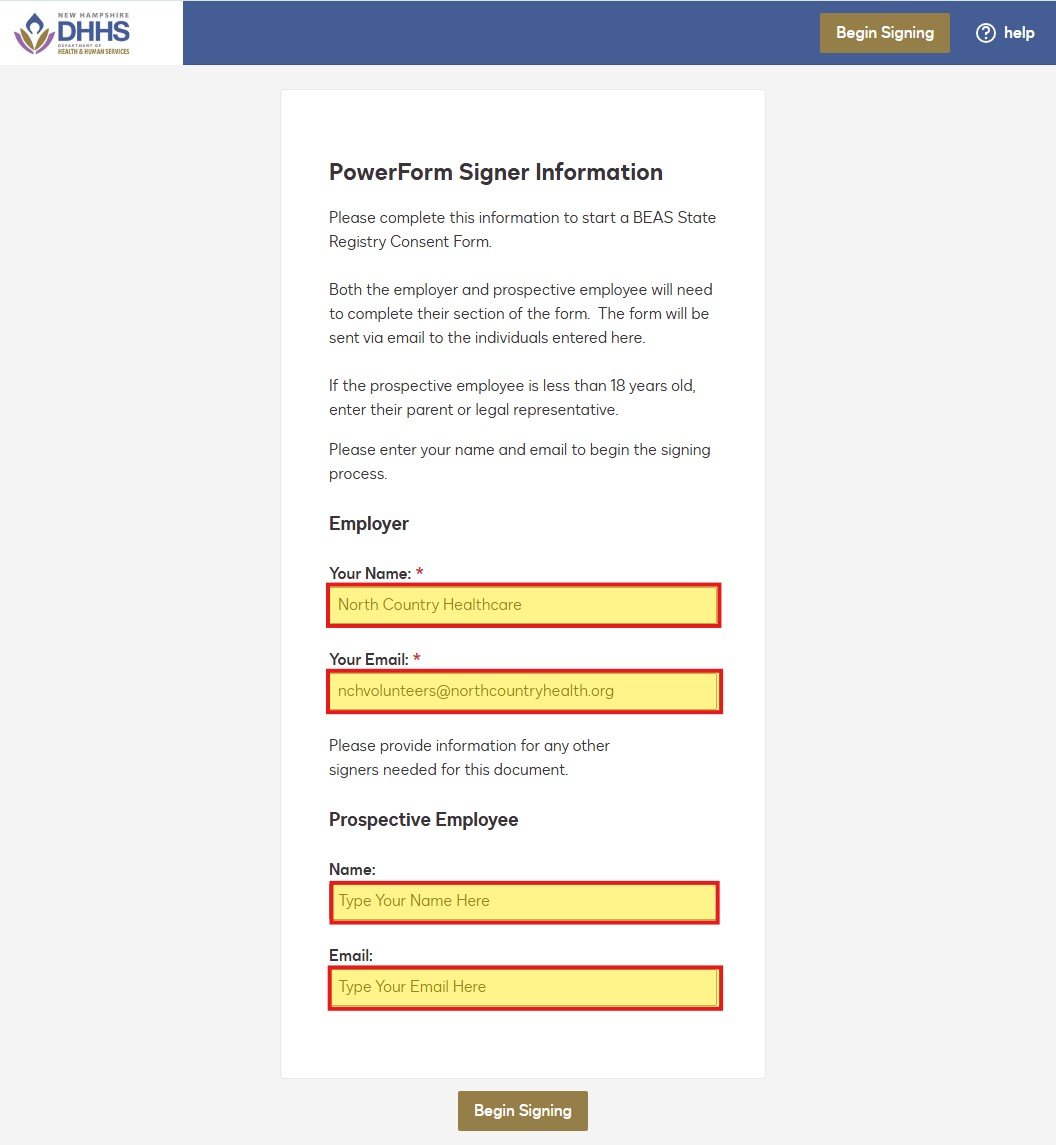
- Employer information as:
- Your Name: North Country Healthcare
- Your Email: nchvolunteers@northcountryhealth.org
- Prospective Employee
- Your Name: Your full name
- Your Email: The same email you used to create your account
See an example below:
Please complete the linked form here.
Copy will be sent to Your Email and nchvolunteers@northcountryhealth.org for review and approval.
